At a Glance
Goals
- Stabilize the fracture
- Reduce pain quickly
- Improve mobility and posture
Timing
- ~30–60 minutes per level
- Walk soon after procedure
- Light activity within 24–48 hours
Best Candidates
- Imaging-confirmed compression fracture
- Symptoms limit daily function
- Limited improvement with meds/bracing
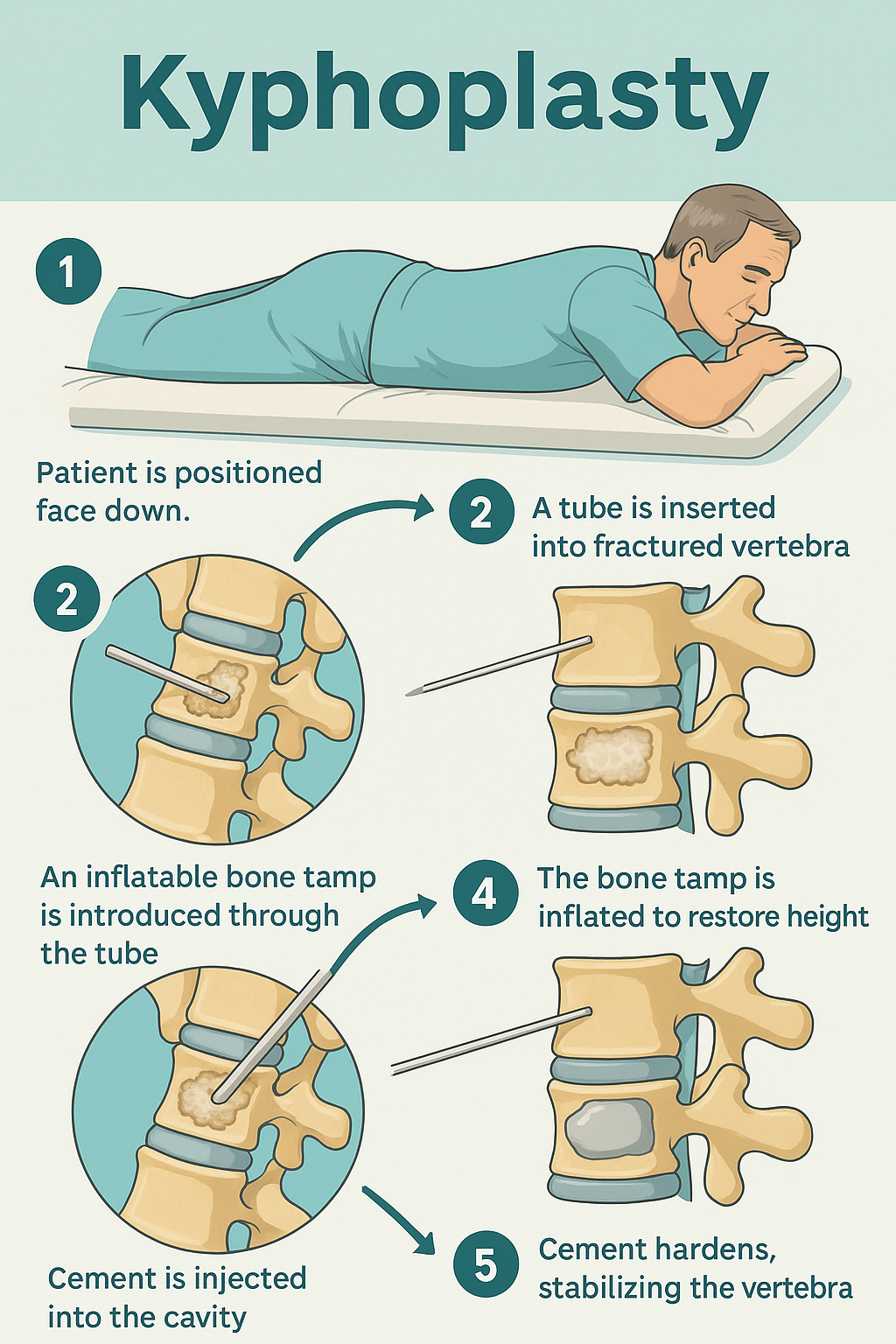
How the Procedure Works
1
Access:
A tiny skin opening is used to guide a cannula into the fractured vertebra under live X-ray.
2
Balloon:
A small balloon is inflated to create space and can help re-expand the collapsed bone.
3
Stabilize:
The balloon is removed and the space is filled with medical-grade bone cement which hardens within minutes.
4
Recovery:
A small bandage is applied; most patients go home the same day with activity guidance.
Benefits & What to Expect
- Pain relief often within 24–48 hours
- Improved ability to stand, walk, and perform daily tasks
- Helps restore vertebral height/alignment
- Small skin opening; stitches usually not required
Outpatient
Quick Relief
Imaging-Guided
- Local anesthesia with light sedation (varies by patient)
- Short observation, then home the same day
- Return to light activity in 1–2 days
- Personalized plan for gradual activity increase
Who’s a Good Candidate?
- Sudden back pain with imaging-confirmed fracture
- Osteoporosis-related fracture not improving with conservative care
- Symptoms that match the fracture level on exam/imaging
- Certain cancer-related fractures after specialist review
Imaging—often X-ray and sometimes MRI—confirms the level and timing of the fracture and aligns findings with your symptoms.
- Earlier evaluation (within weeks) is ideal for decision-making
- Bone-health treatment remains essential to reduce future fractures
Risks & Considerations
- Infection or bleeding (uncommon)
- Cement leakage (usually asymptomatic; rare clinical issues)
- Allergic reactions to materials (rare)
- Sedation-related effects
- Underlying osteoporosis may predispose to future fractures
- Adjacent level fracture risk is largely related to bone quality
- Not all fractures are suitable; timing and pattern matter
Preparation & Aftercare
Before
- Bring recent imaging and a current medication list
- Follow guidance regarding fasting and specific medications
- Arrange transportation home
After
- Keep bandage clean/dry as instructed
- Light activity in 24–48 hours unless told otherwise
- Avoid heavy lifting/twisting until cleared
- Continue osteoporosis management per your clinician
FAQs & Alternatives
Alternatives
- Conservative care: rest, medications, bracing, physical therapy
- Vertebroplasty: cement stabilization without the balloon step
- Specialist-guided cancer or osteoporosis therapies
Is kyphoplasty the same as vertebroplasty?
No. Both use bone cement to stabilize the fracture. Kyphoplasty first creates space with a balloon, which can help restore height before cement placement.
How soon will I feel better?
Many patients notice improvement within 1–2 days; results vary with fracture age, bone quality, and overall health.
Does this treat osteoporosis?
Kyphoplasty treats the fracture. Ongoing bone-health care is essential to lower the chance of future fractures.
How many levels can be treated?
It depends on your imaging and symptoms; your clinician will outline the safest plan.
Educational note: This content is informational and not a diagnosis. Suitability and outcomes vary; your clinician will provide recommendations tailored to you.